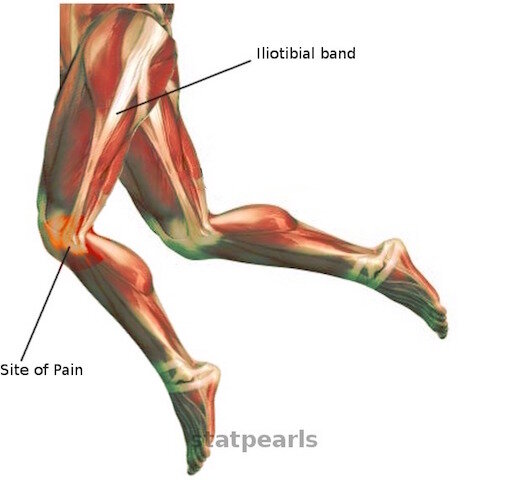
(Image Source: Hadeed and Tapscott)
“Iliotibial band (ITB) syndrome is the most common cause of lateral knee pain in cyclists”
Even though Iliotibial Band Syndrome (ITBS) is more commonly called “Runner’s knee,” don’t let the name trick you, since it’s nearly as common in mountain bikers, triathletes, and cyclists.
The first detailed case of ITBS was published in 1975 and involved military recruits whose running and training activities increased drastically, leading to lateral knee pain.
Iliotibial Band Syndrome is an inflammatory, over-use injury, to the outside of the knee which is caused by a multitude of factors. Drastic or sudden increases in riding intensity or distance are usually to blame and are intensified if you pedal with any anatomical or equipment-related misalignments.
Your iliotibial band can inflame when you flex and extend your knee aggressively and repetitively, which is why it’s common in both runners and cyclists.
“Runner’s Knee” actually refers to two separate over-use injuries
Iliotibial Band Syndrome (ITBS) — Pain on the SIDE of your knee.
ITB = ilio tibial band, which is a band of strong connective tissue or fascia. The ITB runs the entire length of your thigh. ITBS is an inflammation or irritation of this band of fascia
Patellofemoral Pain Syndrome (PFPS) - Pain on the FRONT of your knee or under the kneecap. This is more commonly known as “Biker’s Knee.”
knee pain & IT band syndrome
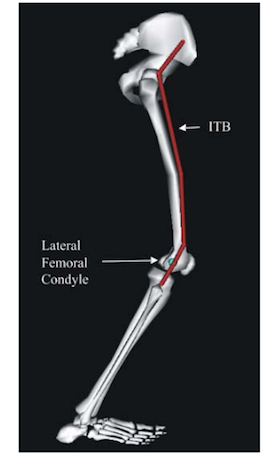
Image Source: (Meardon et al.)
The main symptom of iliotibial band syndrome is a sharp pain on the lateral side of your knee that can radiate into your outer thigh or calf.
The pain is intensified and becomes sharp when your knee is flexed between 20 - 30°
- 30 degrees of knee flexion is known as the “impingement zone,” and it’s at this knee angle you will experience the most discomfort
IT Band syndrome: Compression or friction
There are two general schools of thought when it comes to Iliotibial Band Syndrome:
That ITBS is a friction syndrome and is sometimes called ITBFS, with the F denoting the word friction.
The IT band “rubs” against the lateral femoral condyle
IT Band Syndrome is a compression condition
The femoral condyle moves “under” your IT Band, causing compression between the fibers and layers of fat
Regardless of exactly what’s going on inside your leg, flexion of your knee through the “iliotibial band impingement zone” will cause more pain and further irritate your IT Band.
Even though the most serious pain in felt at 30 degrees, if your IT Band is irritated, it will become even further inflamed with any pedal motions through a knee angle range of 0 to 30°.
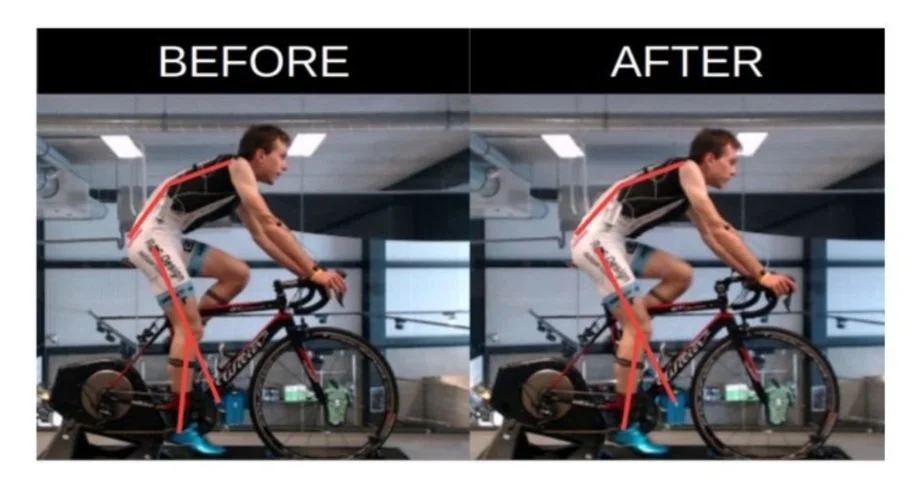
riding with ITB Pain: Optimal Saddle Height
Notice that for “Biker’s Knee,” you raise the seat and for ITBS you lower the saddle- - - (Image source: Bini et al., 2013).
What is the best saddle height to alleviate symptoms from an inflamed Iliotibial Band??
- You need to lower your saddle to allow for a 35° knee flexion angle
- The impingement zone is 30° knee flexion so you need to lower the seat below this point
- Lowering the saddle increases your knee angle
- Keep in mind that faster pedaling will make your hips rock back and forth, which effectively raises your seat height and will require a further lowering of your saddle
However, this is just a temporary solution. This will allow you to continue to train and ride your bike less intensely, without experiencing severe IT Band pain or discomfort but does nothing to address or fix the cause of it.
What causes IT Band Syndrome & cyclists
“A seat that is too high causes excess stretch of the ITB as can improper foot position on the pedal, rigid clipless pedals, and excessively toed in cleats.”
Schematic representation of the anatomy of the iliotibial band (ITB) - - - Image source: (Falvey et al.)
Despite thousands of studies, most notably in runners (after all it’s called “Runner’s Knee”), the exact cause of ITBS is still not fully understood, mainly because ITBS is multifactorial. Meaning, it’s not just one thing that causes your iliotibial band to become irritated or inflamed.
Cycling is very repetitive. During 1 hour of cycling at an average cadence of 60 to 100 rpm, you will spin the pedals 3,600 to 6,000 times. Mixed in with even the tiniest amount of anatomical or equipment-related misalignment, combined with hills, headwinds, or “aggressive” riding, and you end up with a formula for possible dysfunction or pain.
Just a moderately-intense 25 mile (40km) road ride, the average cyclist spends over 8 minutes in the “iliotibial band impingement zone.” That number spikes considerably when you're climbing technical singletrack on your MTB.
A 2017 systematic review from the International Journal of Sports Physical Therapy looked at 72 studies related to cycling and knee pain and determined that ITBS is caused by several factors:
"ITB syndrome is likely caused by increased tibial internal rotation, ITB tightness, inward pointing of toes on the pedals, increased hip adduction, a bicycle saddle position that is too high, and rapid increase in mileage."
Knee pain & Cycling intensity
“The highest prevalence of knee pain (50.0%) was in road racers, but the lowest was in commuters (16.7%), suggesting that the volume and intensity of training are the important risk factors for knee pain”
Cycling intensity and distance are huge factors in the development of Iliotibial Band Syndrome. This makes sense because ITBS is a repetitive stress injury, which is just another way to say overused, overworked, or too much aggressive pedaling.
A study out of Saudi Arabia researched knee problems among cyclists and determined that “high-intensity training was a key factor.”
The research team concluded by saying:
“There was no association with bicycle fitting, coaching, using clip-less pedals, warming up, average years of cycling, average distance ridden in a week, resistance training, strength training, and average rest days in a week."
It is interesting to note that bicycle commuters experience the least amount of knee injuries, while amateur cyclists experience the most. Most commuters ride with flat pedals, regular shoes and clothes, and have their seat set way too low…..so they can put their foot down at stoplights…..basically, they do everything wrong, yet are rarely afflicted with nagging injuries.

optimal saddle height to avoid IT Band syndrome
“15 to 25% of all over-use injuries in cycling are related to the IT Band”
Set your saddle height between 33 - 40° of knee flexion. This will keep your IT Band from “moving” through the impingement zone
Image Source: Korean Journal of Sport Biomechanics
Cumulative Sport Action & IT Band Syndrome
Studies show that if you partake in other repetitive activities, such as running, basketball, soccer, hiking, serious walking, jogging, or backpacking, you are more likely to suffer from ITB syndrome.
If you participate in other activities that have similar repetitive knee extension and flexion, then it’s best to lower your saddle height.
Performing other sports with similar movement patterns strain your IT Band with ITBS developing from the cumulative overload from all these related activities.
straddling the saddle
Just keep in mind that you’re straddling a fine line between a saddle that’s too high or too low.
Let’s not forget that pain in the front of the knee or “Biker’s Knee is from riding with too low of a saddle. Generally, people have about 6% wiggle room between their optimal saddle height and when problems develop. Also, keep in mind that once you combine intensity with long distances, any slight misalignment will be magnified over time.

Performance Coach Jesse - Learn More

Jesse is the Director of Pedal Chile and lives in Valdivia, Chile. Jesse has a Master of Science in Health & Human Performance and a Bachelor of Science in Kinesiology. Hobbies: Mountain biking, bicycle commuting, snowboarding, reading, weight-lifting, taster of craft beers, researcher, & compression sock wearer.
More articles from Pedal Chile









Sources:
Althunyan, Abdullatif K et al. “Knee problems and its associated factors among active cyclists in Eastern Province, Saudi Arabia.” Journal of family & community medicine vol. 24,1 (2017): 23-29.
Balint, Nela Tatiana. “Specific Particularities in the Rehabilitation of Iliotibial Band Syndrome Patients.” GYMNASIUM, vol. XIX, no. 1, 24 June 2019, p. 15, 10.29081/gsjesh.2018.19.1.02. Accessed 21 Oct. 2020.
Bini, Rodrigo Rico, et al. “Effects of Moving Forward or Backward on the Saddle on Knee Joint Forces during Cycling.” Physical Therapy in Sport, vol. 14, no. 1, Feb. 2013, pp. 23–27, 10.1016/j.ptsp.2012.02.003.
Fairclough, John, et al. “The Functional Anatomy of the Iliotibial Band during Flexion and Extension of the Knee: Implications for Understanding Iliotibial Band Syndrome.” Journal of Anatomy, vol. 208, no. 3, Mar. 2006, pp. 309–316.
Falvey, E. C., et al. “Iliotibial Band Syndrome: An Examination of the Evidence behind a Number of Treatment Options.” Scandinavian Journal of Medicine & Science in Sports, vol. 20, no. 4, 13 July 2010, pp. 580–587.
Farrell, Kevin C., et al. “Force and Repetition in Cycling: Possible Implications for Iliotibial Band Friction Syndrome.” The Knee, vol. 10, no. 1, Mar. 2003, pp. 103–109, 10.1016/s0968-0160(02)00090-x.
Flato, Russell, et al. “The Iliotibial Tract: Imaging, Anatomy, Injuries, and Other Pathology.” Skeletal Radiology, vol. 46, no. 5, 25 Feb. 2017, pp. 605–622.
Hadeed, Andrew, and David C. Tapscott. “Iliotibial Band Friction Syndrome.” PubMed, StatPearls Publishing, 2020, www.ncbi.nlm.nih.gov/books/NBK542185/.
Johnston, Therese E et al. “THE INFLUENCE OF EXTRINSIC FACTORS ON KNEE BIOMECHANICS DURING CYCLING: A SYSTEMATIC REVIEW OF THE LITERATURE.” International journal of sports physical therapy vol. 12,7 (2017): 1023-1033. doi:10.26603/ijspt20171023
Meardon, Stacey A., et al. “Step Width Alters Iliotibial Band Strain during Running.” Sports Biomechanics, vol. 11, no. 4, Nov. 2012, pp. 464–472, 10.1080/14763141.2012.699547.
Seo, Jeong-Woo, et al. “Relationship between Lower -Limb Joint Angle and Muscle Activity Due to Saddle Height during Cycle Pedaling.” Korean Journal of Sport Biomechanics, vol. 22, no. 3, 30 Sept. 2012, pp. 357–363.
Walbron, Paul, et al. “Iliotibial Band Friction Syndrome: An Original Technique of Digastric Release of the Iliotibial Band from Gerdy’s Tubercle.” Orthopaedics & Traumatology: Surgery & Research, vol. 104, no. 8, Dec. 2018, pp. 1209–1213, 10.1016/j.otsr.2018.08.013.